Laparoscopic Surgery
Minimally InvasiveSurgery
Case Series
▸ Removal of a 30 kg voluminous ovarian mass, 2023. Original surgical specimen — Prof. Violante Di Donato.
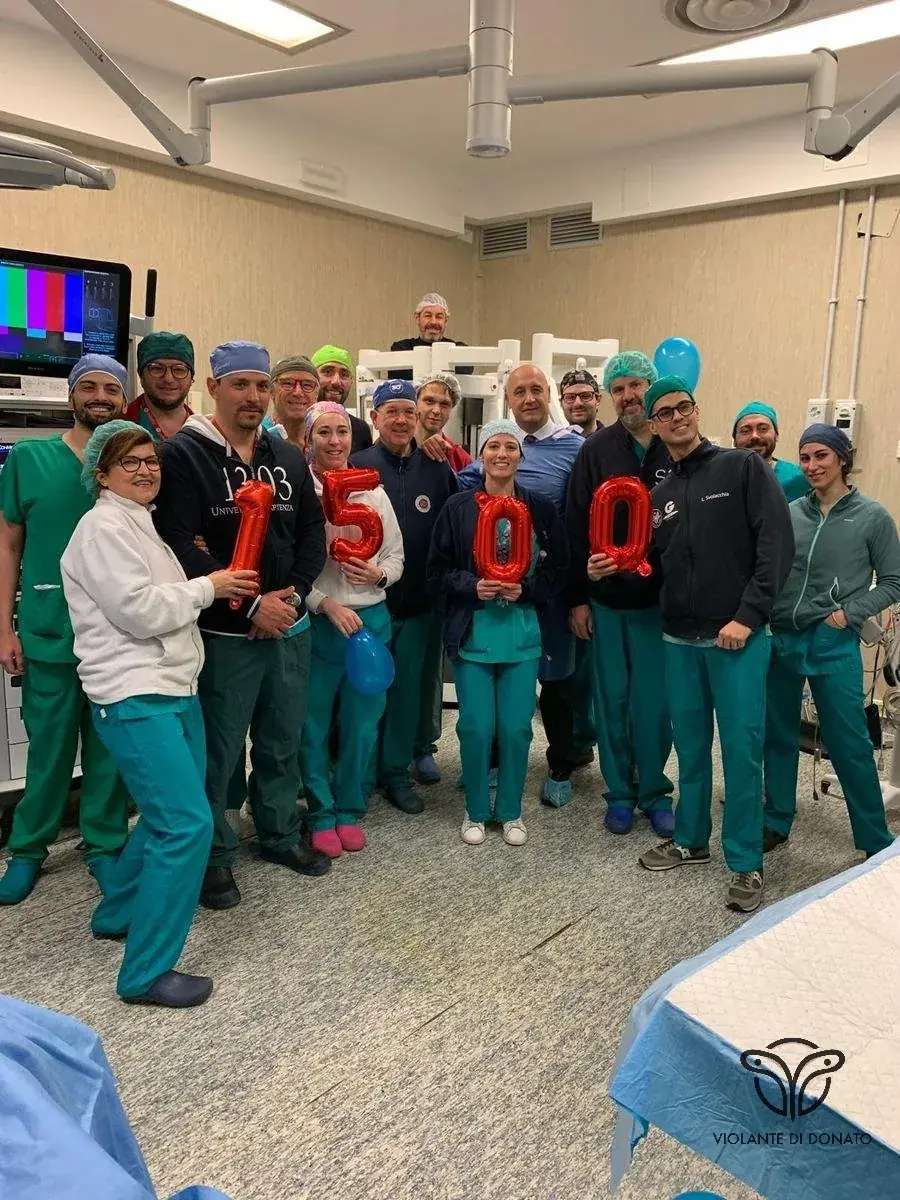
▸ Milestone of 1,500 robotic surgical procedures, Policlinico Umberto I, Sapienza University of Rome. Robotic case series — Prof. Violante Di Donato.
Robotic Surgery
Da Vinci
▸ Da Vinci X Surgical System surgical console. Certified robotic surgery — Prof. Violante Di Donato, Sapienza University of Rome, Policlinico Umberto I.
Hysteroscopy
EndoscopicGynecologic Oncology
Oncologic SurgeryConferences & Training
Academic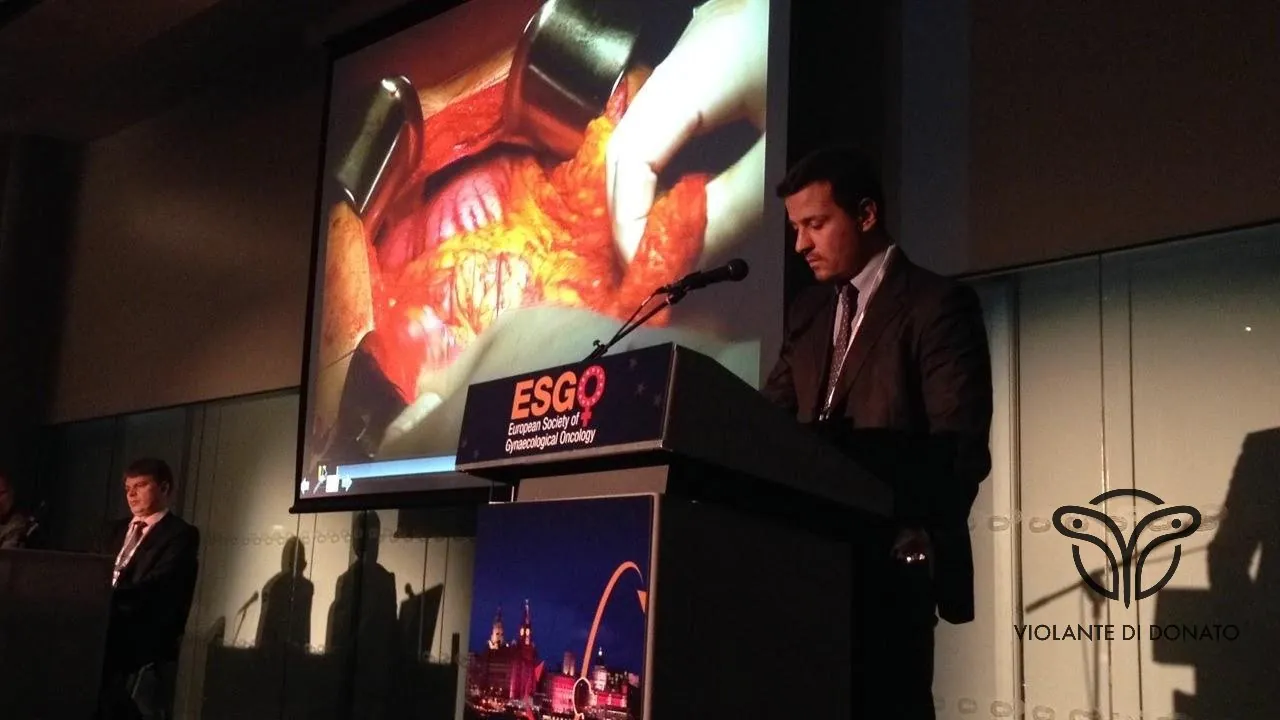
▸ 18th Biennial Meeting of the European Society for Gynaecological Oncology (ESGO), Liverpool, October 2013. Lecture with surgical video — Prof. Violante Di Donato, Sapienza University of Rome.

▸ Public outreach conference at the Italian Chamber of Deputies, Rome. Conference activity — Prof. Violante Di Donato, Sapienza University of Rome.
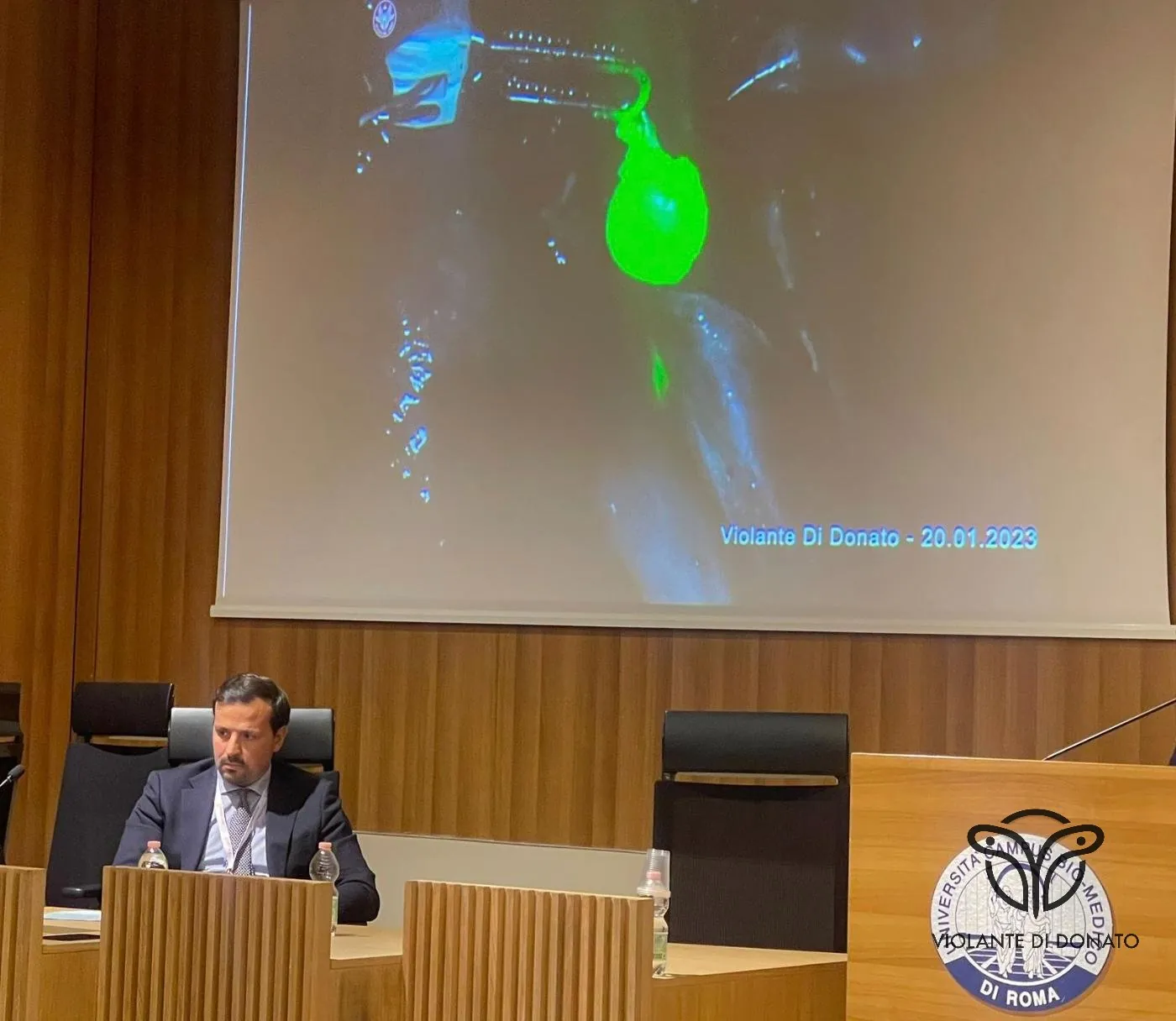
▸ Lectio magistralis on fluorescence-guided surgery, Campus Bio-Medico University of Rome, January 2023. Conference activity — Prof. Violante Di Donato.

▸ Lecture on "Update on the management of persistent HPV infections and CIN". Conference activity — Prof. Violante Di Donato.

▸ International Gynecologic Cancer Society (IGCS), New York, September 2022. International conference activity — Prof. Violante Di Donato.

▸ Lecture on "Updates in endometrial cancer surgery", December 2022. Florence — Prof. Violante Di Donato, Sapienza University of Rome.

▸ Conference "Tailored Gynecologic Oncology — The End of One-Size-Fits-All", Milan, November 30 – December 1, 2023. Lecture on fertility preservation in endometrial cancer — Prof. Violante Di Donato.
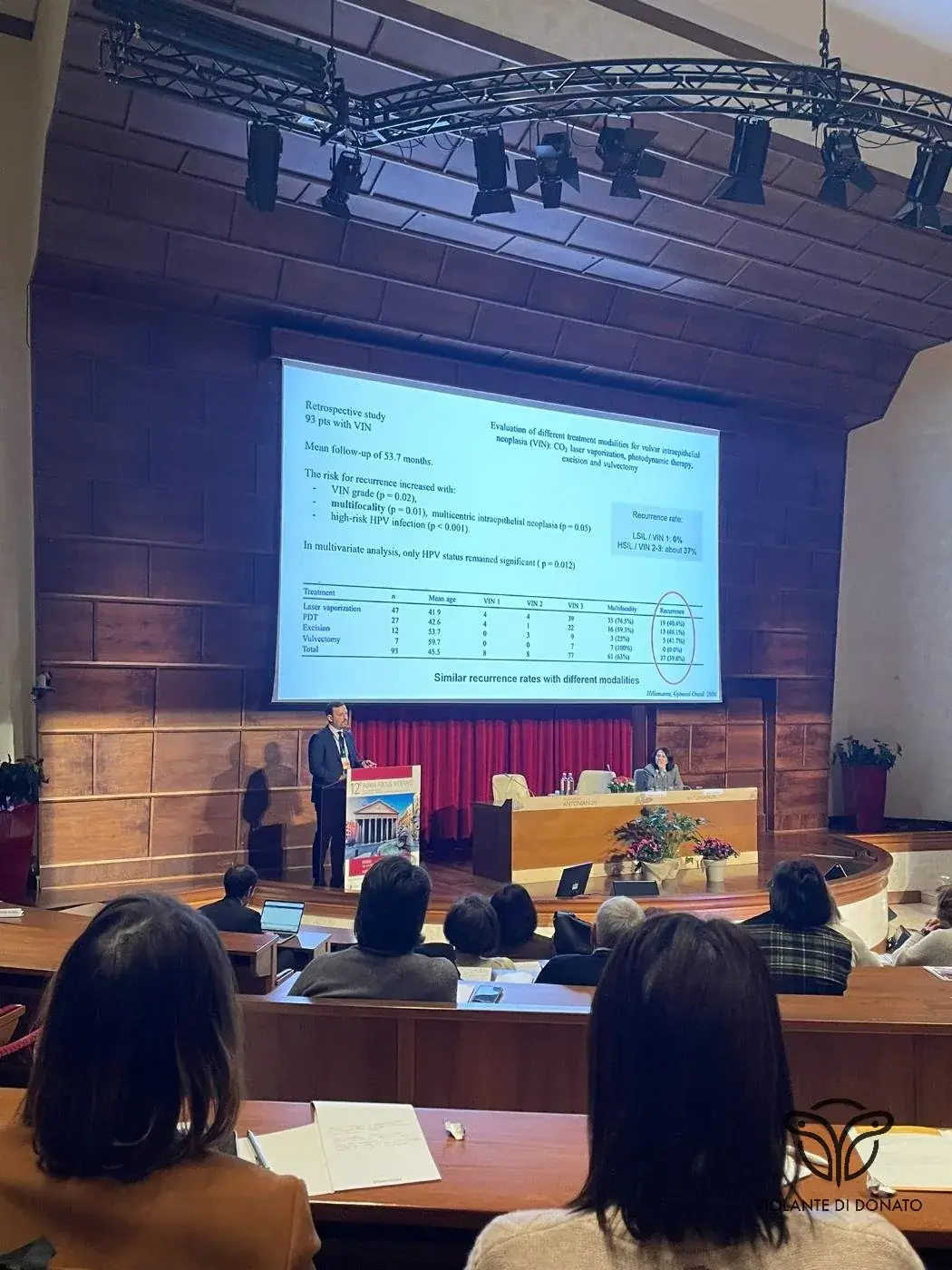
▸ 12th Roma Focus Meeting — Best Clinical Practice in Gynecology, Obstetrics and Reproductive Medicine, February 2024. Lecture on VIN and laser therapies — Prof. Violante Di Donato.

▸ 13th Roma Focus Meeting, Auditorium Antonianum, Rome, February 13–15, 2025. Conference activity — Prof. Violante Di Donato, Sapienza University of Rome.

▸ YMaGiNe Conference "Imaging the Next Steps of Therapy", Milan, December 2024. Lecture on "Evolution of cervical surgery in the Modern therapeutic Landscape" — Prof. Violante Di Donato.

▸ International Congress of Obstetrics and Gynecology "Innovating Women's Health for a Better Future", Tirana, December 2025.

▸ Session "Innovation in Gynecological Surgery — Redefining Standards of Care", Tbilisi, December 2025. International conference activity — Prof. Violante Di Donato.

▸ "Nodi di Cura" Conference — The Future of Gynecologic Oncology between Clinics, Science and Innovation, Milan, November 2025. Chairmanship — Prof. Violante Di Donato.

▸ "Nodi di Cura" Conference, Milan, March 2026. Session on Endometrial Cancer — Molecular Classification. Chairmanship — Prof. Violante Di Donato, Sapienza University of Rome.

Albanian International Delegation

▸ SIGO National Congress, Hotel Ergife, Rome, 2018. Conference activity — Prof. Violante Di Donato, Sapienza University of Rome.

▸ Lecture on PCOS in Sanremo — Banca IFIS, Sanremo, February 2023. Conference and public outreach activity — Prof. Violante Di Donato, Sapienza University of Rome.

Conference Chair greeting from authorities. Sapienza University of Rome, 2023. Conference activity — Prof. Violante Di Donato.

▸ Lecture on the surgical treatment of endometrial cancer, 2023. Conference activity — Prof. Violante Di Donato, Sapienza University of Rome.

▸ Florence Forum — ovarian cancer session, Florence, 2024. Conference activity — Prof. Violante Di Donato, Sapienza University of Rome.
▸ Round Table at the Medical Association of Rome — Prof. Violante Di Donato, Sapienza University of Rome.

▸ Conference at the Medical Association of Rome. Prof. Violante Di Donato, Sapienza University of Rome.
▸ Lecture on management of CIN and HPV-related neoplasms. Medical Association of Rome — Prof. Violante Di Donato, Sapienza University of Rome.

▸ Global Meeting — International Gynecologic Cancer Society (IGCS), Rio de Janeiro, September 2019. International conference activity — Prof. Violante Di Donato.
Best in Women Health Conference, Rome — Prof. Violante Di Donato, Sapienza University of Rome.
▸ Hippocratic Oath ceremony, OMCEO Rome. Institutional activity — Prof. Violante Di Donato, Sapienza University of Rome.
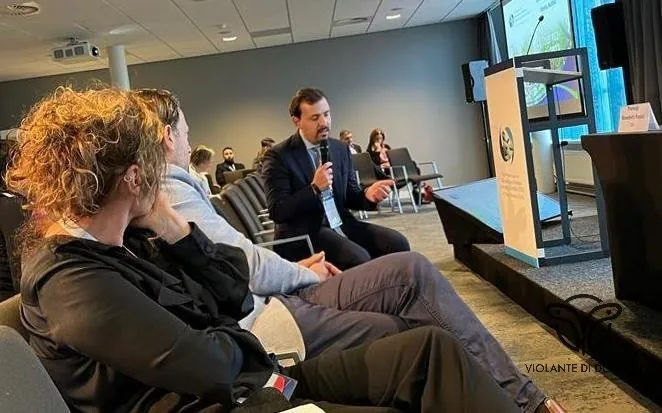
▸ Gynecology panel, 2022. Conference activity — COGI 2022, Amsterdam — Prof. Violante Di Donato, Sapienza University of Rome.
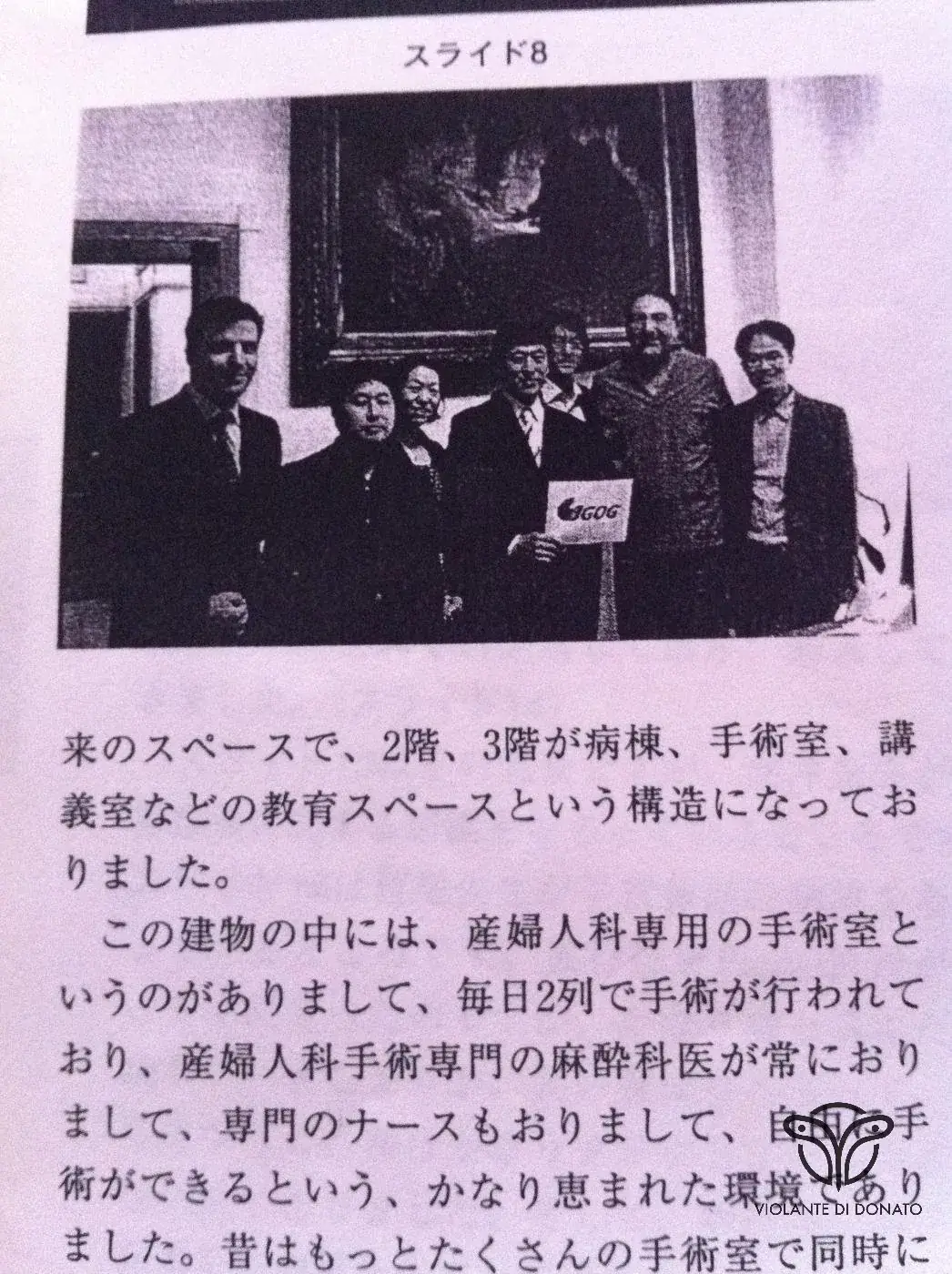
▸ Collaboration with the Japanese Gynecologic Oncology Group (JGOG). International scientific activity — Prof. Violante Di Donato, Sapienza University of Rome.

▸ Keynote lecture in surgical anatomy at Campus Bio-Medico University of Rome. October 2025. Academic activity — Prof. Violante Di Donato.
Media & Interviews
Press & TV
▸ TV interview at the conference at the Italian Chamber of Deputies. Media activity — Prof. Violante Di Donato, Sapienza University of Rome.

▸ Florence Forum 2024 — conference activity collage. Press review — Prof. Violante Di Donato, Sapienza University of Rome.

▸ OMCEO Rome event — Auditorium, HPV and cervical neoplasia session. Media activity — Prof. Violante Di Donato, Sapienza University of Rome.
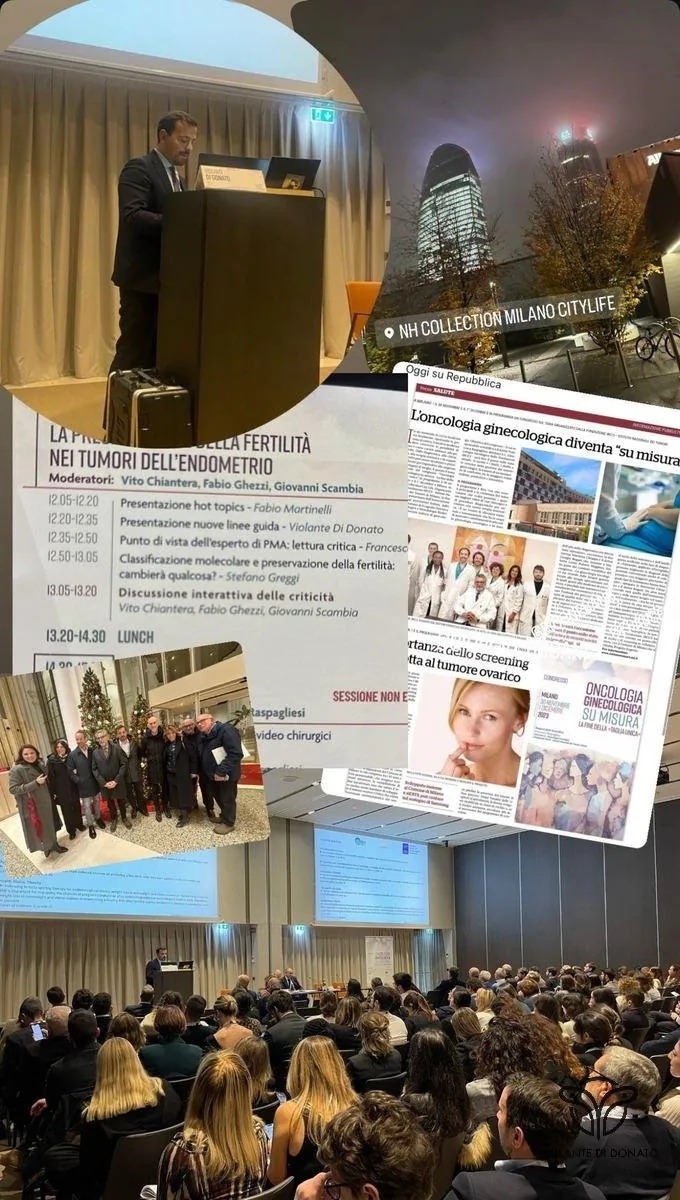
▸ "Tailored Gynecologic Oncology" Conference, Milan 2023 — press and social media review. Media activity — Prof. Violante Di Donato.

▸ 12th Roma Focus Meeting, February 2024 — press review collage. Media activity — Prof. Violante Di Donato, Sapienza University of Rome.

▸ Interview for Top Channel TV at the International Congress of Obstetrics and Gynecology, Tirana, December 2025. International media activity — Prof. Violante Di Donato.