Definition and clinical features
Uterine polyps, also known as endometrial polyps, are generally benign growths arising from the inner uterine wall, the endometrium. They may be attached to the endometrium by a thin stalk or through a broader base of implantation (sessile polyps). The vast majority are benign, although they may be associated with abnormal uterine bleeding, menstrual cycle alterations and reproductive difficulties.
Size is variable, ranging from a few millimeters up to several centimeters in diameter. The highest incidence is observed between 40 and 50 years of age, particularly during the perimenopausal period. Uterine polyps can also be detected after menopause, while they are rare under the age of 20.
In gynecologic practice the endometrial polyp represents one of the most frequent causes of abnormal uterine bleeding and can be diagnosed through transvaginal ultrasound or diagnostic hysteroscopy.
Risk factors
Numerous risk factors are linked to greater exposure to estrogens, hormones that stimulate endometrial proliferation. The risk is increased in the presence of one or more of the following conditions:
- Overweight (BMI 25–30) or obesity (BMI greater than 30)
- Elevated arterial pressure (systemic arterial hypertension)
- Use of tamoxifen, a drug employed in the treatment of breast cancer
- Hormone replacement therapy with high doses of unopposed estrogens
- Genetic predisposition within Lynch syndrome or Cowden syndrome
Symptoms
Uterine polyps may in some cases be asymptomatic, identified incidentally during a routine gynecologic visit or pelvic ultrasound. The principal symptom is abnormal uterine bleeding, which may present with different clinical features.
- Irregular menstrual cycle, with variations in duration or volume of flow
- Menorrhagia (unusually heavy menstrual flow)
- Intermenstrual bleeding (metrorrhagia)
- Spotting or vaginal bleeding after menopause
- Bleeding after intercourse (postcoital bleeding)
- Infertility or difficulty carrying a pregnancy to term
In some cases polyps may protrude through the cervical canal up to the uterine cervix, becoming detectable on gynecologic examination.
Postmenopausal vaginal bleeding always warrants prompt specialist evaluation. In postmenopausal women with bleeding and endometrial polyps, the risk of malignancy is significantly higher than in the asymptomatic population.
Diagnosis
The diagnosis of uterine polyp is based on an integrated gynecologic clinical assessment, including history-taking, specialist examination and targeted imaging studies.
Transvaginal ultrasound
First-line examination that allows visualization of the uterine cavity through an ultrasound probe introduced into the vagina. It enables detection of endometrial irregularities and measurement of endometrial thickness, providing initial information on the presence of intracavitary lesions.
Sonohysterography
Procedure in which a small volume of fluid is introduced into the uterine cavity through a thin cervical catheter, allowing higher-resolution ultrasound imaging of the endometrial walls and any lesions present.
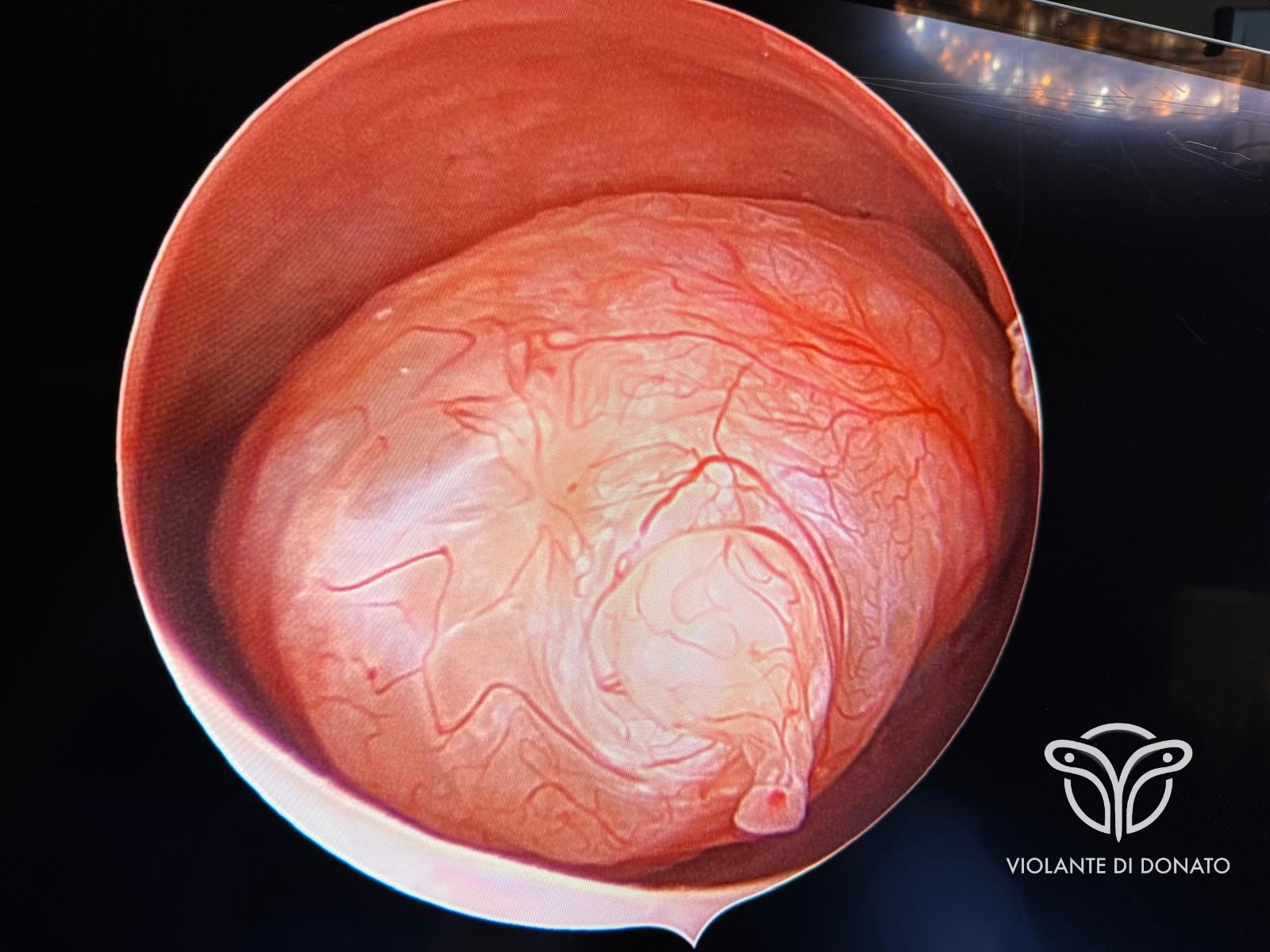
Diagnostic hysteroscopy
This is the reference examination for the study of the uterine cavity. By introducing a small-caliber optical instrument (hysteroscope) through the vagina and cervical canal, it is possible to directly visualize the inside of the uterus and identify polyps, submucosal myomas or other abnormalities with high accuracy. Hysteroscopy can be performed for both diagnostic and operative purposes.
Endometrial biopsy
In selected cases, sampling of endometrial tissue for histologic analysis provides additional information on the nature of the lesion and helps exclude premalignant or malignant changes.
Treatment
The therapeutic approach depends on the characteristics of the lesion, the severity of symptoms, the patient's age and the presence of associated conditions such as infertility or oncologic risk.
Clinical observation
For small polyps in the absence of symptoms, periodic monitoring with ultrasound follow-up may be indicated, without proceeding to immediate intervention.
Pharmacologic therapy
Hormone-based medications — such as progestins or GnRH analogues — may be used to control abnormal bleeding associated with polyps, although they generally do not lead to definitive resolution of the lesion.
Hysteroscopic polypectomy
When polyps cause significant symptoms, abnormal bleeding or interfere with fertility, surgical removal by operative hysteroscopy is indicated. This is a minimally invasive procedure that allows targeted visualization and removal of the polyp without the need for abdominal incisions, often performed in an outpatient setting.
At the end of the procedure, the excised tissue is sent for histopathologic examination, which is essential to confirm the benign nature of the lesion and rule out the presence of atypical or frankly malignant cells.
Hysteroscopic polypectomy represents the reference procedure for the treatment of symptomatic polyps. It allows reduced recovery times, lower organizational impact compared with traditional approaches, and concurrent histologic analysis of the excised tissue.
When to seek specialist evaluation
Specialist gynecologic evaluation should be requested in the presence of abnormal uterine bleeding, unexplained menstrual irregularities, or when a pelvic ultrasound has shown endometrial alterations. Evaluation becomes urgent in the case of any vaginal bleeding occurring after menopause.
Prof. Di Donato provides consultations for cases of abnormal uterine bleeding, suspected endometrial polyps and complex intracavitary disease, including in women with risk factors for endometrial malignancy.
Frequently asked questions
Endometrial polyps originate from the inner lining of the uterus and develop within the uterine cavity, whereas cervical polyps arise from the cervical canal and are often visible on gynecologic examination.
Endometrial polyps are more frequently associated with abnormal uterine bleeding and carry a higher risk of malignant transformation, particularly in postmenopause. Cervical polyps have lesser clinical relevance and a significantly lower risk of malignancy. It has been reported that up to 25% of women with cervical polyps also harbor concomitant endometrial polyps.
Ref.: [8, 9, 10]
Hysteroscopic polypectomy can be performed in an outpatient setting, in most cases without the need for general anesthesia. Office hysteroscopy is considered a safe and effective procedure, with reduced direct costs and lower organizational impact for the patient.
For larger polyps or more complex procedures, local, loco-regional or general anesthesia may be indicated. The choice depends on the size of the lesion, the technique adopted and the patient's individual tolerance.
Ref.: [8, 9]
Endometrial polyps may interfere with fertility, although the mechanism is not yet fully clarified. Proposed mechanisms include mechanical interference with sperm transport, alteration of the endometrial environment and impairment of embryo implantation.
A Cochrane systematic review suggested that the removal of endometrial polyps in women with subfertility may improve pregnancy rates, although further confirmatory studies are needed.
Ref.: [8, 11, 12]
Outpatient hysteroscopic polypectomy is generally followed by rapid recovery. The patient can resume normal daily activities the day after the procedure. Mild bleeding or pelvic discomfort may persist for a few days.
Return-to-work timing and resumption of intense physical activity depend on the surgical technique used, the patient's individual characteristics and the indications provided by the clinician.
Postmenopausal bleeding associated with endometrial polyps always warrants specialist evaluation. Postmenopausal women with bleeding and endometrial polyps have a malignancy risk between 3.8% and 4.93%, significantly higher than in asymptomatic women.
For this reason, in postmenopausal women with bleeding and a suspected endometrial polyp, diagnostic hysteroscopy with removal of the lesion and histologic analysis of the excised tissue is generally indicated.
Ref.: [1, 2, 13, 15]
The recurrence rate of endometrial polyps ranges from 5.6% to 43% depending on the studies and follow-up duration. Factors associated with higher risk of recurrence include obesity, polycystic ovary syndrome, adenomyosis, tamoxifen use, multiple polyps and prior polypectomy.
Ref.: [16, 17, 18, 19, 20]
Histopathology results are generally available within 7 to 14 days from the pathology laboratory, with variations depending on the institution.
Histopathologic examination is mandatory for all removed polyps, as it confirms the benign nature of the lesion and excludes the presence of premalignant or malignant alterations not otherwise detectable.
Ref.: [15]
For information on the gynecologic visit, symptom evaluation and the initial diagnostic pathway, visit the dedicated portal on general clinical gynecology.
iltuoginecologo.it → Clinical gynecology
Specialist Consultation Request
For a clinical evaluation of a uterine polyp or to discuss the indication for hysteroscopic polypectomy, you may request a consultation with Prof. Di Donato.
Book a consultation →